AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2690-8794/005
*Corresponding Author: Martynov V.L, Resident hir. otd. GBUZ BUT
Citation: Martynov V.L, Kolchin D.G, Kurilov V.A, Trukhalev V.A, (2020) Prevention of Reflux Disease After Operations On Gastric And Intestinal Tract, Clinical Medical Reviews and Reports 2(1); DOI: 10.31579/2690-8794/005
Copyright: © 2020 Martynov V This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 17 January 2020 | Accepted: 28 January 2020 | Published: 07 February 2020
Keywords: surgery, reflux, complications, “plug” on the small intestine
Creating anastomoses between the hollow organs of the abdominal cavity, abdominal formations of the retroperitoneal space and the jejunum always raises the question of preventing reflux from the jejunum into the drained cavity of the esophagus, stomach, gallbladder, external hepatic ducts, cysts of the liver and pancreas. After surgery, any reflux becomes pathological. Reflux is an obligate precancer. Thus, the reflux of bile and pancreatic juices in the stomach, the stump of the stomach and esophagus contributes to the occurrence of reflux esophagitis, reflux gastritis, ulcers and gastric cancer or its stump. After internal drainage of the cavity formation in the jejunum, postoperative reflux disease develops, which is caused by the actions of the surgeon who tried to help the patient sincerely. This allowed such states to be defined as “iatrogenic postoperative reflux disease”.
The purpose of this work was to develop and introduce into practice the “plug” on the resulting loop of the jejunum, which does not migrate into the lumen of the intestine, with internal drainage of the hollow organs of the abdominal cavity and abdominal formations of the retroperitoneal space and evaluate the clinical results.
As a result, the authors have developed a method for creating a “plug” on the jejunum loop, which is used for drainage, studies are being conducted on its safety, adequacy of functioning, general accessibility, and clinical situations are analyzed. For drainage of the abdominal formation impose a fistula between it and the jejunum loop 40–50 cm from the ligament of Treitz. We form an inter-intestinal fistula according to Brown, above which the length leading to a drained formation of the area of the jejunum is about 10 cm, in the middle of which we impose a “plug”. The length of the small intestine section which diverts from the drained formation to the inter-intestinal brown anastomosis is about 30 cm.
To form a “plug”, we use the free area of the greater omentum, through which we perform a ligature of non-absorbable polypropylene material by vcol-vykola. The developed method of forming a "plug" does not cause abrupt ischemic changes in the area of operation, followed by necrosis of the intestinal wall and migration of the "plug" into the intestinal lumen, and its effectiveness has been proven using clinical observations, microcirculation studies, water test results and X-ray examination. The method of creating a "stub" is promising for the internal drainage of abdominal cavity formations and retroperitoneal space, for the formation of areflux nutrient eunostoma.
Creating anastomoses between the hollow organs of the abdominal cavity, the retroperitoneal space and the jejunum always raises the question of preventing reflux from the jejunum into the drained cavity of the esophagus, stomach, gallbladder, external hepatic ducts, cysts of the liver and pancreas. After surgery, any reflux becomes pathological. Thus, the reflux of bile and pancreatic juices in the stomach, the stump of the stomach and esophagus contributes to the occurrence of reflux esophagitis, reflux gastritis, ulcers and gastric cancer or its stump. Reflux is a precancer [1–3]. The current stage of development of gastric surgery is characterized by a critical assessment of the long-term results of gastrectomy and the search for new, physiological, technical aspects of the operation [4]. The creation of esophago-enteral anastomoses always raises the question of preventing the reflux of intestinal contents into the esophagus. Impact on the mucous membrane of the esophagus of intestinal contents unusual for it, which is possible during gastrectomy and extirpation of the stomach in various modifications, inevitably contributes to the occurrence of reflux esophagitis [5, 6]. This complication is regarded as severe functional pathology of the operated stomach and occurs, according to different authors, in 19.2–95.4% of cases [1, 7, 8].
Most methods of forming an esophageal-intestinal anastomosis are aimed at increasing its reliability and do not provide for the creation of an anti-reflux mechanism that provides physiological, batch evacuation of food [9, 10]. Prevention of functional impairment after gastrectomy is estimated as an exceptional parameter for improving the quality of life of patients who have undergone an already complicated surgical procedure [8, 11].
During gastrectomy, the inter-intestinal anastomosis during Balfour surgery reduces the incidence (30–75%) and the severity of enterogastric reflux compared with those using the Hofmeister – Finsterer method, but does not completely prevent it [12]. In this study, many authors show that the length of the discharge loop of the intestine should be at least 80-100 cm. Only an abdulent segment of the intestine sufficient in length (80-100 cm) significantly reduces intestinal reflux, which reduces the likelihood of developing ascending cholangitis [3, 13, 14]. At the same time, it is known that in the mobilized along the Roux loop of the small intestine with a length of more than 40 cm the probability of the development of stasis syndrome sharply increases. Therefore, the length of the discharge loop of more than 40 cm during resection according to Roux is attributed to the main risk factor for the development of stasis syndrome; a loop length of 35–40 cm is considered optimal [5]. In order to combat these refluxes, Chaput, in 1895, crossed the lead loop between the anastomoses. To prevent reflux, Y-shaped anastomoses were formed. The most widespread operation in the modification of Ru, but it has its drawbacks: it is necessary to completely cross the intestine, which causes additional infection of the abdominal cavity, microcirculatory changes in the wall of the loop of the intestine, cut out by Roux; the intersection of nerve fibers in 9–50% of cases causes Ru-staz syndrome [5, 15, 16].
The number of patients with diseases of the pancreatoduodenal zone, extrahepatic bile ducts, which are accompanied by the development of obstructive jaundice, increases every year [17–19]. The formation of biliodigestive anastomoses causes free communication of the bile ducts with the gastrointestinal tract (GIT), changes the rhythm of bile secretion and creates conditions for ascending infection in the biliary system, leading to the development of reflux cholangitis in 0.7–21.1% of patients, and scarring formed intestinal anastomoses occurs in 9.8–28.0% of cases [20–23]. When performing reconstructive operations with an extended or high stricture of the common bile duct, preference is given to biliodigestive anastomoses with the small intestine turned off from the Roux or Brown passage [24–27]. Internal drainage of pancreatic cysts (RV) in the gastrointestinal tract has become the most common, its frequency of use reaches 80% [28-30, 51]. Of all cystodegative anastomoses, preference is given to the formation of fistula with the jejunum on the disconnected loop according to Roux, Brown or Shalimov [31]. In order to prevent the throwing of intestinal contents in practice, the most commonly used method is the formation of a “stub” proposed by Professor A.A. Shalimov [32, 33], which consists in a laparotomy, the selection of the afferent loop of the small intestine to the drained structure, which is tied up with two ligatures. Instead of ligating the intestine with ligatures, it can be stitched with a lung root suturing clamp (UKL) and then invaginated with sero-serous sutures. However, the authors themselves point to a possible restoration of the patency of the intestinal canal due to the pressure sore of the ligatures. Their invagination also not always can reliably prevent the restoration of the intestinal lumen. A bedsore depends on the ischemia of the intestinal wall in the place where the ligatures or clips of the UCL apparatus are applied.
The imposition of cystopancreatojejunostomy with the intestinal loop not turned off from the passage of the chyme is unacceptable [34]. Creating an anastomosis with the jejunum turned off from the transit of food masses significantly reduces the risk of infection of the cyst cavity [35].
Thus, after internal drainage of the hollow organ into the jejunum when a chyme gets into it, postoperative reflux disease develops, which is caused by the actions of the surgeon who tried to help the patient sincerely. This allowed such states to be defined as “iatrogenic postoperative reflux disease”. To prevent bedsores and restore the anatomical patency of the jejunum at the site of imposition of the "plug" should be excluded compression of the tissues of the small intestine.
Creating nutritional eunostomy. The proportion of patients with nutrient enterostomy is 3.3–8.0% among patients with intestinal ostomy [32, 36]. Such negative effects of enterostomy as dehydration, electrolyte disturbances, as well as local parastatic manifestations limit the use of this operation. However, the number of patients who need enterostomy formation does not decrease [37, 38].
Nutritional eunostoma surgery of the esophagus. Enteral nutrition (EP) has indisputable advantages over parenteral nutrition [39, 40]. The use of enteral nutrition through areflux to an adynamic preoperative period in exhausted patients with prolonged obstruction of the esophagus helps stabilize the body's anabolic processes, restore the visceral and partially somatic pool of proteins, normalize the ratio of protein fractions, improve immune status, thereby more adequately prepare the patient for radical surgery. In the postoperative period, early enteral alimentation contributes to a more rapid activation of intestinal motility, reduces the number of infectious complications [39-41].
Tumor stenoses and cicatricial strictures of the esophagus lead to obstruction of the proximal digestive tract with the development of alimentary insufficiency, exhaustion and extinction of the compensatory abilities of the body [42], which causes the rejection of the simultaneous formation of an artificial esophagus in patients of this category.
Conducting EP through the areflux valve valve in patients with cancerous stenosis of the esophagus can be the method of choice for preoperative preparation and postoperative management [43]. Enteral nutrition through areflux enostomy has all the advantages of parenteral, has fewer complications. In addition, areflux valve eunostoma allows not only to feed the patient, but also to keep the stomach suitable for further plastics [42]
Nutritional eunostoma in gastric surgery. V.D. Fedorov (2008) reported five observations of patients [44] who, due to continued bleeding after conservative treatment, endoscopic and a number of surgical interventions (gastrotomies with suturing erosions and ulcers, resections and resections of the stomach) against the background of deep anemia and hypoproteinemia were forced extirpation of the stomach stump was made. Due to the severity of the condition of the patients, the operations were limited to the removal of the gastric stump without the imposition of esophagoenterostomy. These operations were completed by external drainage of the abdominal segment of the esophagus and the imposition of Yeunostoma according to Maidl for subsequent enteral feeding. Thanks to intensive treatment, three out of five patients survived. After 4–6 months, he performed reconstructive surgeries with imposition of the esophago-intestinal anastomosis along Roux.
The most effective method of treating patients with duodenal stump failure is the drainage of the stump area in combination with enteral tube feeding [45]. The use of the Y-shaped eynostoma for these purposes made it possible to reduce mortality by 2 times.
Nutritional eunostoma in biliopancreatoduodenal surgery. Oncological diseases of the biliopancreatoduodenal zone account for 3.6% of the total oncological structure and reach 11.5% among the malignant neoplasms of the gastrointestinal tract with a frequency of involvement in the pathological process of the pancreas, reaching 63–86% [6, 34].
Pancreatoduodenal resection is the main method of radical surgical treatment of tumors of the pancreas, but is accompanied by the development of severe postoperative complications [46], the most frequent of which are the divergence of the sutures of the pancreatojejunal anastomosis, the development of acute postoperative pancreatitis, multiple organ failure; mortality reaches 50% [13, 47, 48].
Nutritional eunostoma in mediasthenitis surgery. The problem of increasing the efficiency of treatment results in patients with acute perforation mediastinitis for many years remains an urgent task [50].
I.V. Yurgelas (2009) found that jejunostomy provides antireflux protection, enteral nutrition, gastrointestinal decompression and treatment of intestinal insufficiency syndrome and in the complex treatment of acute perforation mediastinitis allows for 3.72 times lower mortality rates, the frequency of registration of both isolated complications and the development of their complex combinations [48].
The purpose of the study is to develop and introduce into practice the “plug” on the resulting loop of the small intestine, which does not migrate into the intestinal lumen, with internal drainage of the hollow organs of the abdominal cavity and abdominal formations in the retroperitoneal space.
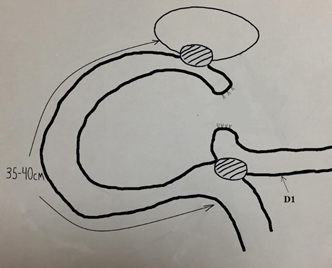
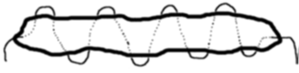
For drainage of the abdominal mass, a fistula is placed between it and the jejunum loop 40–50 cm away from the Treitz ligament. Form inter-intestinal fistula according to Brown. The length leading to the drained formation of the jejunum area from the inter-intestinal anastomosis is about 10 cm, in the middle of which a “cap” is placed. The length of the region of the jejunum which diverts from the drained formation to the inter-intestinal Brownian anastomosis is about 30 cm (Figure. 1).
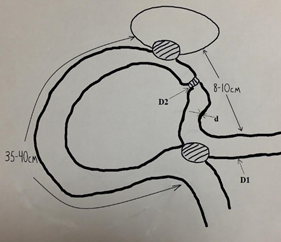
We form a "plug" on the small intestine according to the developed method, in which compression and necrosis of the small wall are excluded, followed by migration of the "plug" into the intestinal lumen. As can be seen from the operation scheme, the principle of drainage according to Roux remains, but without crossing the intestine, nerve pacemaker fibers (there is no threat to the development of Roustaz syndrome), without additional infection of the abdominal cavity (Fig. 1 - A, B, C).
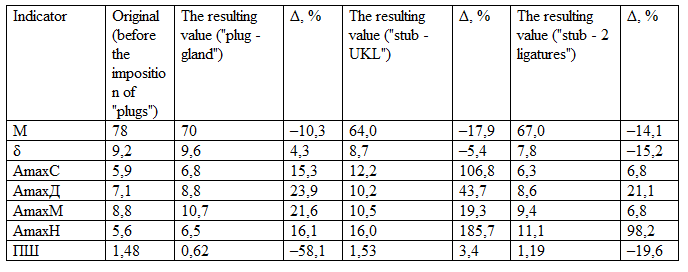
For the formation of the “plug”, a free area of the greater omentum is used, through which a ligature of non-absorbable polypropylene material is carried out by vcol-vykola (Fig. 2).
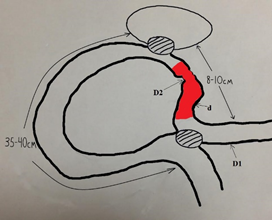
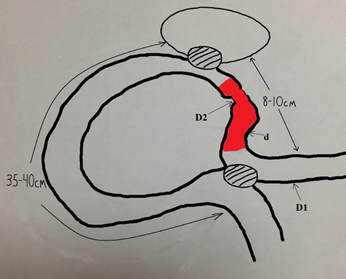
To exclude reflux, a 2–5 cm distal to the intestinal anastomosis from the afferent loop is 2-5 cm distal to the intestinal fistula and a “plug” is applied according to the developed procedure, in which compression and necrosis of the small intestine wall are excluded (RF patent No. 2253379) with subsequent migration of the “plug” into the lumen of the intestine (Figure. 3).

For the imposition of "plugs" by the developed method during the operation, the caliper of the jejunum wall d is determined by a caliper (divided into 2 thickness of the matched opposite walls) and the diameter of the section of the small intestine D1, on which the "plug" is planned. Upon receipt of the desired parameters, the required diameter of the “plug” is calculated, and thus the corrugated portion of the jejunum is calculated using the formula D2 = 2 D1d, after which the intended operation stage is performed (RF patent №2253379): d is the thickness of the jejunum wall; R1 is the radius of the small intestine; R2 is the radius of the corrugated portion of the small intestine; D1 is the diameter of the jejunum; D2 is the diameter of the corrugated section of the small intestine by a “stub”; S1 = 2πR1 - the cross-sectional area of the wall of the small intestine; S1 = 2πR1d = D1πd; S2 = πR22 = π (D2 / 2) 2 - the cross-sectional area of the corrugated wall of the small intestine; S1 = S2 - the condition of the absence of compression, ischemia and necrosis of the wall of the small intestine in the area of "stub"; D1πd = π (D2 / 2) 2; D2 / 2 = D1d. The construction of the “plug” is formed from a free insulated section of the greater omentum, through which a ligature of non-absorbable polypropylene material is drawn by injecting a stick. This complex is placed on the small intestine, the ends of the thread are tied with the formation of a ring with a diameter of D2.
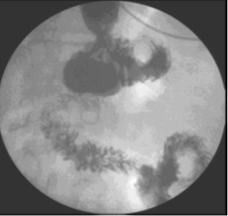
The obtained possible intraoperative values of the wall thickness of the small intestine, its diameter and the obtained required diameter of the “plug” according to the formula (RF Patent No. 2253379 (authors Martynov V.L., Kolchin D.G., Buldakov D.I. , Bodrov AA)) are combined in a table (Table 1).

Using the developed table, it is not necessary to spend time on mathematical calculations. After measuring the wall thickness of the jejunum and its diameter, comparing the results, we find in the table the required diameter of the “plug” and form it surgically in accordance with the size found.
Determination of the state of the microcirculatory bed of the intestinal wall of the "plug" zone in the experiment
The evaluation of microhemodynamics with various methods of forming an intestinal anastomosis was carried out by laser Doppler flowmetry on the LAKK-02 apparatus (NPP Lazma, Russia) in an experiment on 10 white-down rabbits (age 1.5–2.0 years), which were formed by three "plugs" on the jejunum: two ligatures (the first) and the apparatus of the UKL according to А.А. Shalimov (the second) and the developed method (the third).
Water sample. The study was performed on 15 anatomical preparations, then - on 15 rabbits. According to the developed formula with the use of a non-absorbable ligature and the free strand of the greater omentum, a “plug” was placed on the small intestine with the calculation of the absence of ischemia of the intestinal wall. At 10–15 cm from the “plug”, a soft intestinal press was applied. Between the pulp and the "plug" created a closed space. Water was injected into the lumen of the intestine between the “plug” and the clamp through a needle until the voltage of this section of the intestine was significant, and the possible passage of water through the “plug” zone was evaluated.
X-ray examination. In the immediate postoperative period, fluoroscopy of the anastomosis area with passing barium was performed with normal radiographs (see Figs. 5, 6) to normalize the condition. The study was performed in 57 (83%) patients.
The clinical application of the method was carried out in the surgical department of the State Budgetary Healthcare Institution “GKB No. 12 of Nizhny Novgorod” The criteria for inclusion in the study group were the formation of a “plug” on the jejunum during the drainage of the hollow organs of the abdominal cavity and abdominal formations of the abdominal space in various pathologies. The study group consisted of 155 patients aged from 20 to 78 years. Among them were 53 (34%) men and 102 women (66%).
The nature of the diseases for which patients are operated to drain cavities with the formation of a “plug”: pancreatic cysts - 15, stomach cancer - 13, chronic violation of duodenal permeability - 92, liver cysts - 2, pancreatic head cancer, mechanical jaundice - 21, Vater papilla cancer, obstructive jaundice - 10, strictures of extrahepatic bile ducts - 7, rupture of the lower thoracic esophagus, mediastinitis - 1, pancreatic cancer and stomach with high obstruction, which required the position of nutritious areflux yeunostomy - 4.
During examination in the clinic, patients were diagnosed with comorbidities (for a number - combined comorbidities): bronchial asthma - in 52, diabetes mellitus - in 5, urological and gynecological pathology (urolithiasis, chronic adnexitis) - in 3, hypertensive disease and CHD - in 4, vegetative dystonia syndrome - in 39, chronic tonsillitis and pharyngitis - in 37, peptic ulcer of the stomach and duodenum - in 51, chronic calculous cholecystitis - in 20, chronic colic stasis - in 12, rheumatoid arthritis t - at 3, skin disease (psoriasis, neurodermatitis, eczema) - at 36.
This procedure was used in the following operations: in 15 cases - in the drainage of pancreatic cysts, in 5 - in the case of gastroenterostomy, in 5 - in the case of gastroenterostomy after gastrectomy, in 3 - in the case of esophagiojejunostomy after gastrectomy, in 92 - with duodenojejoneostomy, in 2 - with drainage of liver cysts, in 21 - with cholecystojejunostomy, in 7 - with reconstructive operations on the biliary tract, in 1 - with the imposition of a “plug” on the cervical esophagus (instead of ligation) with its perforation and development of mediasthenitis, in 4 - for the formation of ares luxurious nutritional stoma.
Clinical observations. The duration of observation of the operated patients was from 1 to 5 years. In no case was the migration of the created construct into the lumen of the intestine or specific complications noted. In five cases, after repeated relaparotomy for other diseases, the formed structure adequately fulfilled its functions, being the system that was originally created, while in five clinical observations (the operation to create a “plug” modified by AA Shalimov was carried out in other medical institutions ) “Plug”, created using the UKL apparatus, was not found in the places of its formation and isolation of the drained cavitary formation was not achieved.
Microcirculation study. In the area of "plug - gland with a ligature" microcirculation (MC) decreased by 10.3%. In the area of "plug - UKL" between the lines of clips MC was absent. In the area of "plug - ligatures" MC between the threads was also absent. That is, there is a great risk of necrosis of the intestinal wall between the lines of the clips and between the ligatures with possible dangerous consequences. In 1 mm aside from the line of formation of the “plug - UKL” of the MC decreased by 17.9%, in 1 mm of the “plug of the ligature” of the MC decreased by 14.1%. In the zone of each "stub" marked venular stasis. In the “stub” zone with an epiploon, all compensatory mechanisms for the normalization of the MCs were activated (Table 2).
Results of water test. In no case did the passage of water through the zone of the formed “plug”, both in the experiment and in all 155 clinical intraoperative studies, were noted (Fig. 4).
The results of x-ray examination. In no case was the flow of barium into the drained structure. The contrast stopped in front of the “plug”, which was guaranteed not to let intestinal contents through this intestinal segment.
Indicator Initial (before imposition of "plugs")
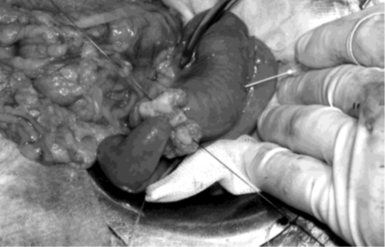
We give an example of the clinical functioning of the “plug” on the jejunum adductor loop to the esophagus after gastrectomy. On a series of X-ray images, no barium passage through the jejunum segment in the place of the formed “plug” was detected. The contrast goes to the leading part of the jejunum only to the “stub” zone. The main part of the contrast goes through the outlet gut (Fig. 5, 6). Thus, it has been proven that the esophagus is isolated from the damaging effects of bile, the digestive juices of the duodenum and the pancreas.


1. The developed method of forming a “plug” does not cause abrupt ischemic changes in the area of operation, followed by necrosis of the intestinal wall and migration of the “plug” into the intestinal lumen.
2. The formed “plug” according to the developed method in practice does not guarantee that the chyme passes through this intestinal segment.
3. The method is safe, widely available, adequately performs the intended areflux function.
4. The method of creating a “stub” is promising for the internal drainage of the hollow organs of the abdominal cavity and abdominal formations of the retroperitoneal space, for the formation of areflux nutritional ejunostoma
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
